 English
English  Turkish
Turkish  German
German  Spanish
Spanish 
Fill out the form and we’ll call you!
In order for revision surgery to be performed, the following must be pre-sent:
– The patient has had a previous obesity surgery,
– The previous surgery did not make the patient lose enough weight,
– After the surgery, the patient lost weight, but the patient gained weight again,
– Have an unsuccessful surgery
However, it should be known that the anatomy of the patient may have changed after the operation, and the revision surgery to be performed on the patient may be more complicated and risky than the first. In this case, the knowledge and experience of the operating doctor is very important.
Some questions need to be answered before deciding on revision surgery:
It is important to answer the following questions in determining why the first operation failed.
– Why could not the patient lose enough weight?
– Did the surgeon who performed the first operation have sufficient expe-rience?
– Did a problem occur in the surgical technique?
– Has the patient’s eating habits changed after the first operation?
– What is the patient’s alcohol or carbohydrate consumption?
– Has the patient adapted to the nutrition program given after the surgery?
– Has the patient applied an exercise program after the surgery?
– Does the patient have any medications or hormonal disorders?
– Was the first operation performed on the patient a correct operation method that would make the patient lose enough weight?
– How is the patient’s stomach volume and structure now?
– Was there any intervention in the intestines in the first surgery?
After these questions are answered, the patient’s revision surgery is de-cided. After the previous surgery, the decision of which surgical procedure will be performed in revision surgery is very important.
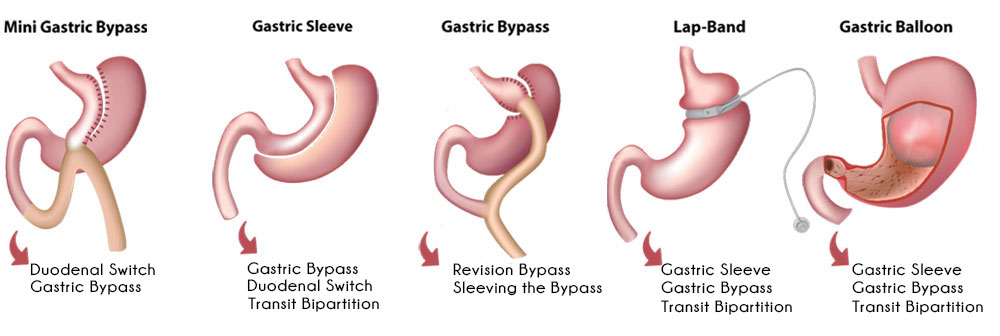
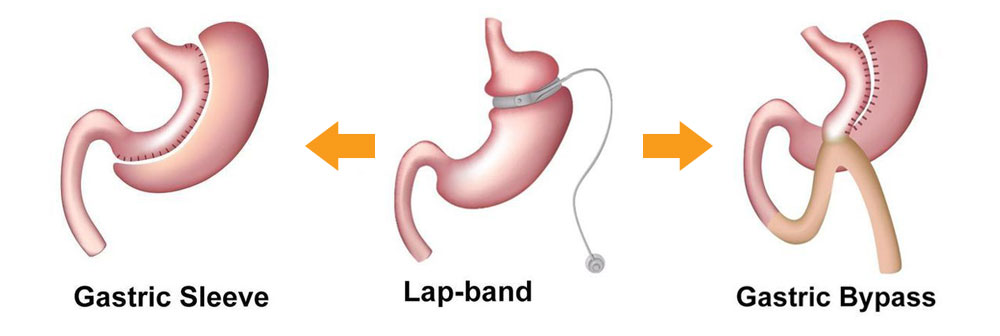
For example, operations that can be applied as revision surgery to a pa-tient who has previously been applied gastric banding; gastric sleeve, gastric bypass, transit bipartition, sadi-s surgeries.
In this case, it should be determined how much weight the patient needs to lose, and it should be considered whether the patient has diabetes.
The revision surgery of the patient who had a sleeve gastrectomy has always been the subject of discussion. If the patient has an enlarged stomach or if there is a stomach that was not removed sufficiently during surgery and therefore remained wide: sleeve gastrectomy can be applied to the patient a second time. However, if there is an unexpanded stomach, gastric bypass, transit bipartition, sadi-s, mini gastric bypass operations can be performed on the patient.
It is very important to determine the stomach diameter of the patient in de-ciding which surgery will be performed. The reason why the patient gained weight should be revealed in detail. In revision surgeries, this information is used in planning the surgery method that the patient will not regain and lose enough weight.
If the patient has undergone gastric bypass surgery, dumping syndrome may have occurred, the patient may be losing too much or too little weight. For these reasons, revision surgery can be performed. For example, if there is a dumping syndrome problem after gastric bypass, revision sur-geries that will enable the gastrointestinal anastomosis line to be reconsid-ered should be preferred. However, if the patient has not been able to lose much weight after gastric bypass surgery, moving the anastomosis line to the distal region (taking it down) may be the solution. Or, if the patient has lost a lot of weight, approaches that will lengthen the absorbing surface of the stomach in revision will be more beneficial in order to keep the absorp-tion area longer.
As can be seen, a very good decision should be made in line with the pa-tient’s problems, just like playing a game of chess. Phrases such as “The revision of sleeve gastrectomy is xxx surgery” cannot be used be-cause there are many alternative solutions to sleeve gastrectomy and the surgeon must find the most accurate solution and apply it.
The response of a revision surgery is to transfer the first operation of the patient to another obesity surgery. The second method should be a non-failure, targeted, uncomplicated, solution-oriented approach.
